
“After the death of my husband I had the feeling being thrown into a new world. A world where I can see people smiling like I used to do, but unable to imitate this behavior. A world where I lost the ability to feel feelings like the people around me. A world where every food has the same taste: nothingness. A world where I see that my family is suffering due to my changes. ”
There is no one who understands me since I’m in another world. In addition to this I’m feeling physical sick. I’m feeling pain. I can’t sleep at night but I’m tired, tired of this life everything is hurting everything is uncomfortable I just don’t want to breath anymore just don’t want to go on with this. Not a day goes by that I’m not feeling pain in every part of my body that I’m not feeling uncomfortable. I can’t see an end from all of this. I just want it to end. If I would know a solution I would take it. But I don’t see one so the only thing I can think of day in day out is ending it by myself.” This is an attempt to give an insight on what are the thoughts of a lot of people are who are suffering from a depression. Depression is nowadays a widespread disease. It’s hard these days to still find a person who neither had depression and/or doesn’t know someone close to him who had depression once in their life. But if we talk about depression we need differentiate between different types of depression. But before we do this we first need clarify something about mental illnesses:Mental illnesses are not a 0 - 1 state!
It’s not you either have depression or you don’t. Either you have schizophrenia or you don’t. But rather it is a spectrum. The thing is psychologists need to define a threshold which defines at which point the disease is so severe that you have to treat this person. If the threshold is to low, you will have too many patients who will come to the psychologists which will bring a couple of problems. Just imagine which problems would arise if people would went to the doctor because of every little complaint they have. On the other hand if the threshold is too high you will find a lot of people who are sick and yet don’t get any treatment because the definition says they are not sick enough. So you get the point. But of course you could always argue about these definitions. Some find them to low others too high. But what’s important for us to keep in mind is that these definitions are not absolute. Some people might not have by definition a depression and yet they are in a state where they need help. Same applies on the other hand: some people might have by definition a clinical depression and yet they can handle it all by themselves.
Regarding the latter case I would like to clarify something. If you either had/have depression, know someone who have/had depression or you just dealt with the topic you most likely heard already the following sentence or even might thought or said it yourself:“Just get yourself together”
Or something similar like this (e.g. “Just stop being sad”, “try to have a positive mood” etc.). Just a short question: How helpful do you believe is it to say to someone who just had a car accident and is screaming out of pain “get yourself together” or “just ignore the pain” because (and here comes the point):“It’s only in your brain”
Because that’s where our pain is! Physical and emotional pain is both rooted in our brain and not in our arm or any other area.
You will find that people with a depression (depending on the kind of depression) will have physical changes in their brain. So it’s not that simple to just “change your thoughts and be happy”. There are certain types of depression where it is possible to change certain behaviors in your everyday life in order to fight this disease. But even in these cases a simple “change your thoughts” will most likely not be helpful. Rather having a structured approach in dealing with this calamity will be helpful.
I assume that this is also one of the reasons why you will often hear from people who are suffering from depression (especially major depressive) sentences like:“As long as you didn’t experience a depression by yourself, you never can fully get it”
And I hold that sentence to be true, since their brain is working differently compared to a brain from a person without depression (reading this sentence keep in mind what I said early: mental illness is not a 0-1 state; it’s not that you either have depression or not).Definition of depression
Ok, so how is depression defined in a clinical context? First of all there are different types of depression and their definitions vary mainly depending on their duration and intensity. But all of them are part of what is called
Mood affective disorders
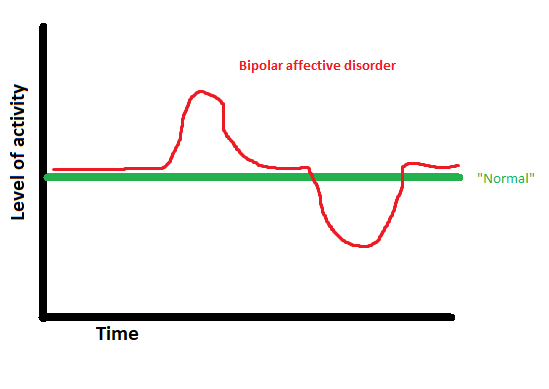
Mood affective disorders are characterized by abnormal changes of the mood. These changes are either in the direction to depression or to elation and they differ regarding being acute, episodic and chronic. What’s critical is the level of activity (i.e. abnormal high activity/elation -> mania, abnormal low activity -> depression). This part is important to understand.
Depression is not mainly/necessary about being sad but rather being in state of just not wanting to do ANYTHING.
| There was a case of a woman who experienced an event in her life which afterwards led her to just stare at a white wall for hours. It’s hard to say that she’s sad at that moment. But it’s obvious that she just went into “standby-mode”. |  |
A mania is the opposite of that. So the person having a mania is basically overactive. Since this article shall be about depression I will at this point not go any further into details. If you desire a more detailed explanation of a mania let me know in the comments.
In the following you’ll see an overview of mood affective disorders.
Disclaimer: The following graphics are only for illustration purposes! The shown gradients can also look differently: differentiating in intensity, duration, frequency and order (order: regarding bipolar affective disorders).
- • Manic episode

- • Bipolar affective disorder
- • Depressive episode
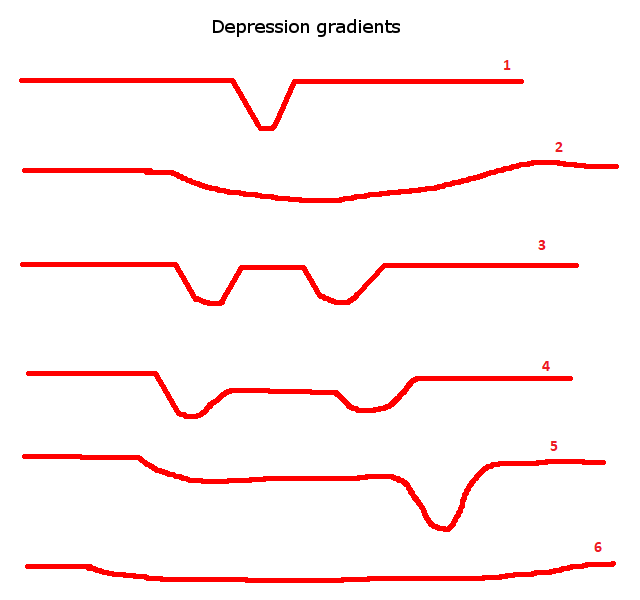
- In order to make this graph more untestable here are three examples (number 1, 2 and 4):
1. Single depressive episode
2. Chronical single depressive episode
4. Recurrent depressive episodes without full remission between the intervals
Manic episodes as well as bipolar affective disorder also have different types of gradients, which I will as said early not go into further details.
Regarding depressive episodes you can see that there are a lot of different types of gradients. These different gradients are not just a matter of definition, but rather it plays a crucial role for a person who experiences this disease on how he experiences it. Furthermore it plays also an important role on how the disease will be diagnosed and how the treatment will look like.
Healing procedure
If a person is suffering from depression the procedure of healing will look similar to any other disease:
- 1. The person needs to feel sick
- a. Possible problem: a lot of people don’t realize that what they have is a sickness so they might have feelings of guilt and that it’s their fault that they’re always sad and not in the mood of doing anything. What enhances this might be the environment and the people around them; making them accusations that they’re always down and they should get themselves together or might even cut the contact to them and leaving them all alone.
- 2. Going to the doctor
- a. Possible problem: in a LOT of cases people go to the doctor due to a physical complaint yet the root of it is a psychological. What often happens is that the doctor is not able to identify any sickness and leaves the patient with the information that he’s actually healthy. Leading again to the feeling that it’s the fault of the patient and that he imagines these troubles. Alternatively the patient is going to the doctor multiple times up until the doctor is diagnosing him with hypochondria since the patient is describing pain for which there is no physical evidence.
- 3. If however the doctor realizes that the patient might be suffering from a mental illness he might direct him to a trustworthy psychologist.
- a. Possible problem: Money and time. Psychologist are usually very expensive, so it is no surprise that even if you know that you have a mental illness chances are that you just cannot afford it to get a treatment. The other problem is that even if you can afford it, you might still need to wait a couple of month just to get an appointment.
- 4. Treatment
- What I'd like you to know about the treatment:
- a. You need to change certain things by your own. It’s not sufficient to go to the doctor and expect him to just heal you. You need to change certain behaviors under the guideline of the psychologist.
- b. Problem here is that it is of utmost important to have a trustworthy psychologist. Someone who knows what he’s doing. Some might just give you medications right away and that’s it. Some might just give you a treatment which they personally prefer and not the one which suits you best.
- c. You need to know that it takes time! It will take more than a weekend course or a youtube video or a steemit post for that matter to treat this disease.
- 5. Post-treatment
- a. Possible problem: is that the depression comes back. If you got a good treatment chances should be reduced of a relapse (but not eliminated). So that’s another reason why it’s important to take time and effort in looking for a trustworthy psychologist.
If after all of this you now think that you have a depression (which often happens when people read about diseases, psychological or physical) here is a screening from the American and Depression Association of America (ADAA):
https://www.adaa.org/iving-with-anxiety/ask-and-learn/screenings/screening-depression
But PLEASE independent of the outcome DON’T FREAK OUT. It’s just a screening. If you truly believe that you need professional help first ask trustworthy people about your situation and then make your decisions.
If you enjoyed this article and were able to take some benefit out of it, I’ll appreciate it if you upvote, comment and resteem it. Furthermore I appreciate it as well if you follow me @sharing-thoughts if you enjoy these kinds of articles.
----------------------------------------------------------------------------------------------------------
For further information:
http://apps.who.int/classifications/icd10/browse/2016/en#/F30-F39